 |
Original Article
Visual acuity and contrast sensitivity outcomes based on photoreceptor layer after retinal reattachment surgery
1 Department of Ophthalmology, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
Address correspondence to:
Andi Muhammad Ichsan
Department of Ophthalmology, Faculty of Medicine, Hasanuddin University, Makassar
Indonesia
Message to Corresponding Author
Article ID: 100002O02AI2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Ichsan AM, Tajuddin AS, Muhiddin HS, Budu, Umar BT, Waspodo N. Visual acuity and contrast sensitivity outcomes based on photoreceptor layer after retinal reattachment surgery. Edorium J Ophthalmol 2019;2:100002O02AI2019.ABSTRACT
Aims: To evaluate correlation between photoreceptor layer thickness with visual acuity and contrast sensitivity in primary retinal reattachment after vitrectomy.
Methods: Twenty seven eyes of 27 patients (mean age 45.6±12.7 years) with successfully retinal reattached were analyzed. Snellen chart visual acuity (VA) to evaluate best-corrected visual acuity (BCVA) converted to the logarithm of the minimum angle of resolution scale (logMAR) and contrast sensitivity in photopic and mesopic illumination using Lea Symbol Flip Chart, funduscopy examination and High Definition Optical Coherence Tomography (HD-OCT) were used to measure retinal condition and photoreceptor layer thickness.
Results: Nineteen (70.4%) cases of total 27 cases were reported with macularon RRD. The thickness of the photoreceptor layer was 43.8±10.8 µm which was significantly correlated with BCVA (logMAR 0.3-2.4, mean 1.0) with p <0.005 and also with contrast sensitivity in mesopic with p 0.033 (p ≤ 0.05). Contrast sensitivity in photopic was better than in mesopic. Foveal anatomic abnormalities were detected in six eyes (22.2%), that was disruption of inner segment (IS)/outer segment (OS) junction and also disruption of external limiting membrane (ELM). Duration of detachment also significantly correlated with BCVA with mean 36±29 days. The macular status before surgery determines the quality of vision, whereas the macular-on rhegmatogen retinal detachment gives visual acuity, contrast sensitivity, that is better in both photopic and mesopic, than macular-off.
Conclusion: Photoreceptor layer thickness significantly correlated with visual acuity and contrast sensitivity in mesopic illumination, whereas thicker the photoreceptor, better the visual acuity and mesopic contrast sensitivity.
Keywords: Contrast sensitivity, Inner segment (IS)/outer segment (OS) junction, Rhegmatogenous retinal detachment
INTRODUCTION
Recently, surgical techniques and equipment for retinal reattachment allow higher success rate of retinal detachment management resulting better visual outcomes even in cases of macular-on or macular-off rhegmatogenous retinal detachments (RRD) [1],[2],[3],[4]. However, some cases showed poor anatomical results that include epiretinal membranes, pigment migration, cystoid macular edema, and retinal folds [5],[6],[7].
In these cases, subtle changes in the foveal structure, which may cause visual disturbances, can hardly be identified during standard clinical examinations such as slit-lamp biomicroscopy or binocular indirect ophthalmoscopy.
The introduction of optical coherence tomography (OCT) provides a new way to obtain objective data of clinically hidden retinal structures. OCT has led to many new findings in studies of retinal abnormalities, especially of macular disorders [8],[9],[10]. Sometimes, the retina had already anatomically reattached as confirmed with indirect ophthalmolscopy [11],[12],[13]. Even after successful retinal reattachment and normal OCT findings, however, postoperative vision may be unsatisfactory in some cases despite good visual acuity [14]. Such patients may report poor visual function that cannot be detected by visual acuity tests. Contrast sensitivity is an index capable of assessing visual function more sensitively than visual acuity [15]. It was known that the longer the duration of macular detachment, the smaller the increase in contrast sensitivity in patients after RRD surgery [16]. However, no reports have addressed contrast sensitivity in patients with primary retinal reattachment in mesopic and photopic illumination. The purpose of this study was to assess the correlation between photoreceptor layer thickness with visual acuity and contrast sensitivity photopic and mesopic in primary retinal reattachment after vitrectomy.
MATERIALS AND METHODS
The present study was an analytic observational study with cross-sectional design conducted in Hasanuddin University Hospital and Celebes Eye Centre, Makassar, Indonesia. The subjects who met the inclusion criteria were patients with primary retinal reattachment after vitrectomy pars plana. Any additional ocular diseases affecting central visual function including severe macular degeneration, history of past retinal surgery and ocular trauma were considered in exclusion criteria.
Data collection
All patients who met the inclusion criteria were informed about the study procedure and if they agreed then they were asked to sign the consent application. Twenty seven patients were included in our study. Preoperative data were age, sex, preoperative bestcorrected visual acuity (BCVA) using Snellen chart converted to the logarithm of the minimal angle of resolution (logMAR), time from the onset of symptoms to surgery, lens status, macular status, vitreous substitutes. Patients had a complete ophthalmologic examination including measurement of BCVA, contrast sensitivity, intraocular pressure using Goldmann applanation tonometry, slit-lamp examination, and dilated fundus ophthalmoscopy.
Contrast sensitivity
Contrast sensitivity was measured using LEA numbers flip chart with three meters distance in two conditions, photopic with illumination level 85 cd/m2 (85 lux) and mesopic with illumination level 3 cd/m2 (3 lux). Illumination level was determined using luxmeter. Chart presents numbers at the following contrast levels: black, 25%, 10%, 5%, 2.5%, and 1.25%. Each level consists of five numbers. The result was based on the number of patients who could see.
HD-OCT imaging
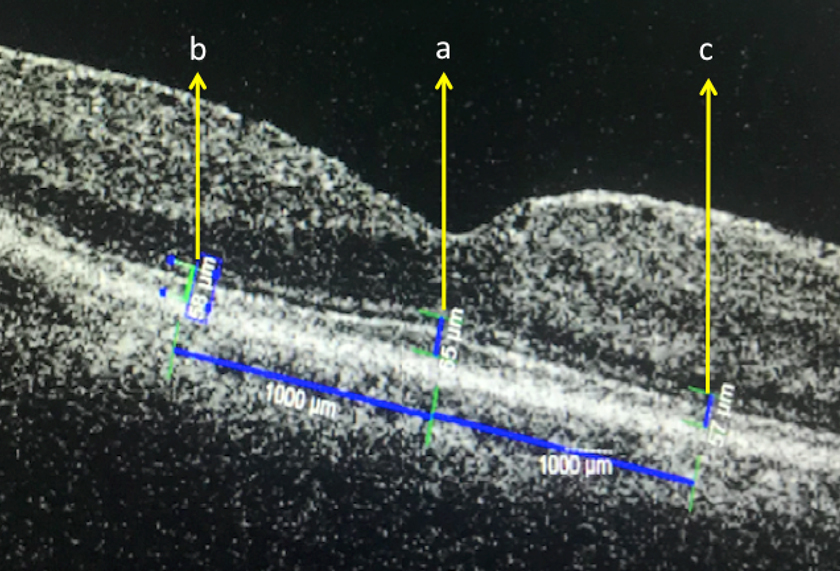
The entire macular area was scanned with an HDOCT instrument (Cirrus OCT; Carl Zeiss Meditec) with scan lengths of 9 mm for horizontal scans and 6 mm for vertical scans. High-quality images were obtained by using the five-line raster mode and en face analysis for IS-OS junctions. The distance between the inner border of the ELM and the ellipsoid zone (EZ),which had previously been called as the photoreceptor IS and OS junction line, was taken to be the IS thickness, and the distance between the EZ and the inner border of the retinal pigment epithelium (RPE) was taken to be the OS thickness. Photoreceptor thickness was taken from IS and OS thickness and measured in three locations : at foveola, 1000 µm nasal foveola (perifovea 1), and 1000 µm temporal foveola (perifovea 2). Central foveal thickness is distance from ILM to RPE thickness that was made on the OCT images passing through the fovea. This was made with the software of the system (Figure 1). Scans with a signal strength of >7/10 were considered appropriate, and a representative image was selected for the measurements.
Data analysis
All data obtained was recorded and data analysis was performed using Statistical Package for Social Science (SPSS) version 22. The analysis method used was descriptive and analytic (statistical test). For statistical tests, Spearman rho correlation coefficient and comparative Mann Whitney U test were used. The test results were considered significant if the p value was <0.05.
RESULTS
Twenty seven eyes from 27 patients were included in the study. There are 12 men and 15 women with 18 samples in right eye and 9 samples in left eye. Of 27 patients, 19 patients had macular-on RRD, and 8 patients had macular-off RRD. Based on lens status only 3 patients had phakic eyes and remaining were pseudophakic. All patients underwent vitrectomy pars plana surgery to attach the retina with silicon oil as vitreous substitutes and only one patient with gas C3F8.
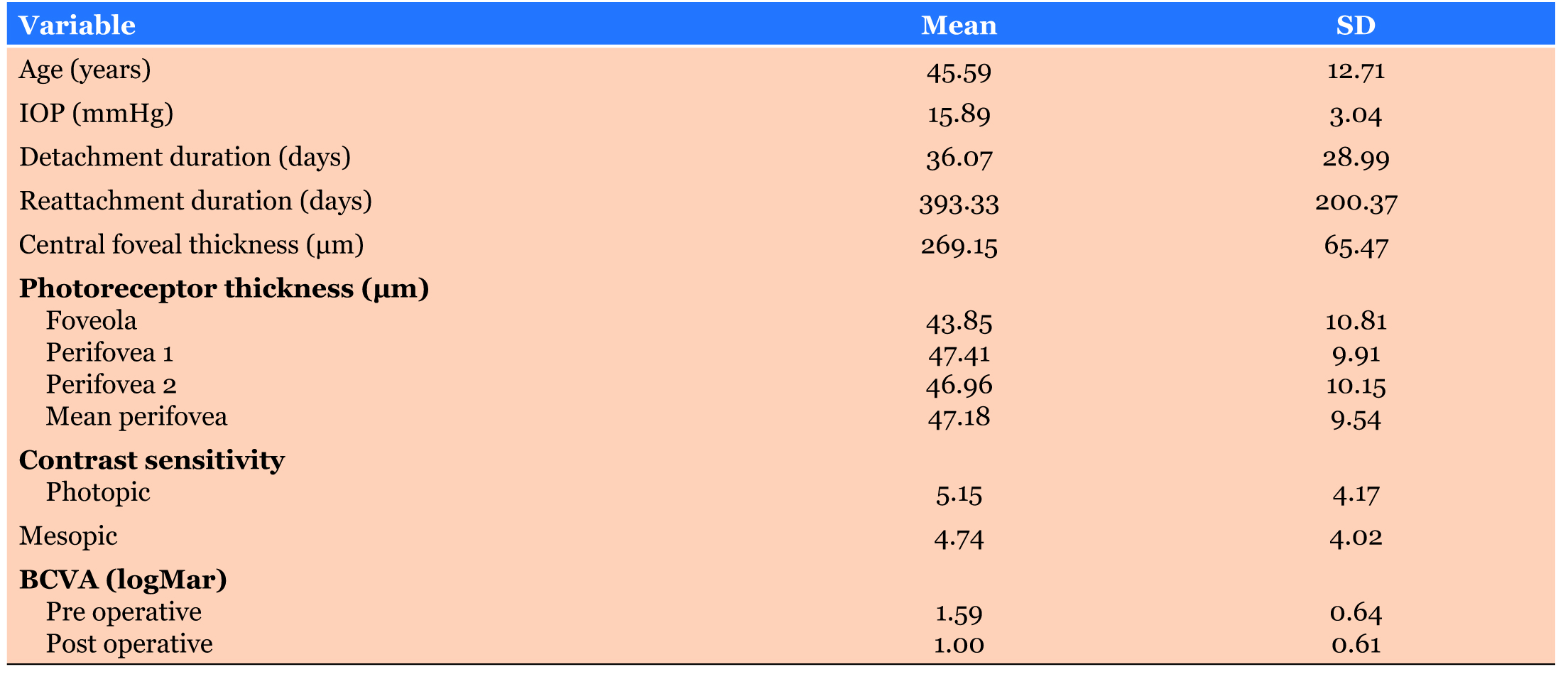
Characteristics of patients are shown in Table 1. Mean age was 45.59±12.71 years with duration of detachment 36.07±28.99 days. Best corrected visual acuity (BCVA) preoperative had logMAR mean 1.59±0.64 (range : 0.7- 2.7) and post-operative with logMAR mean 1.00±0.61 (range : 0.3-2.4). Central foveal thickness was 114–418 µm with mean photoreceptor thickness at foveola was 43.85±10.81µm
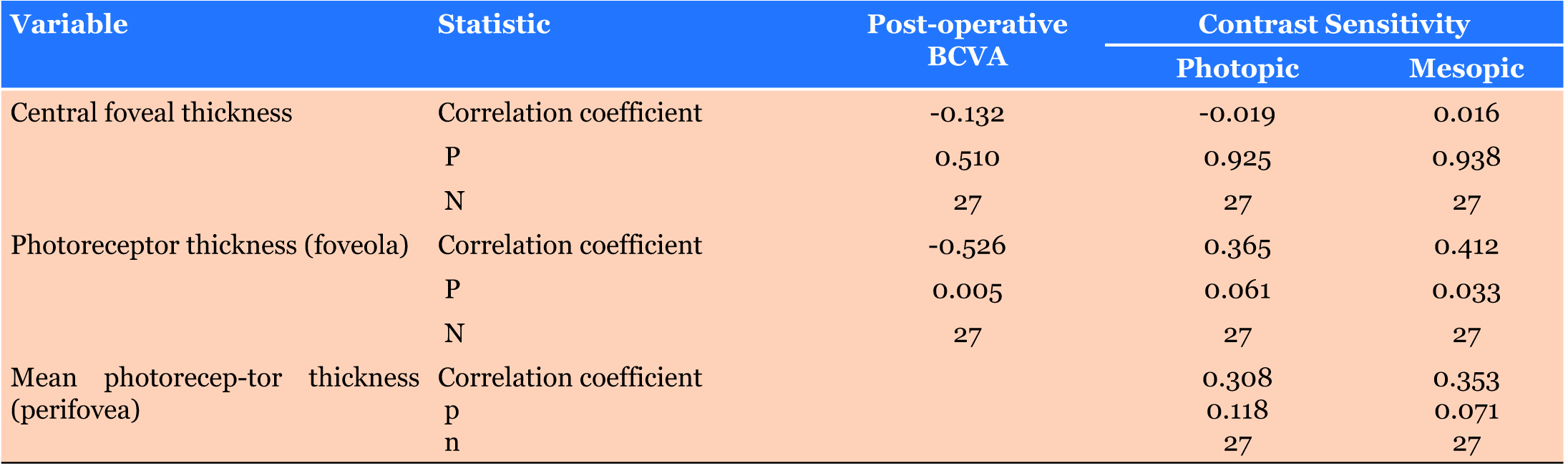
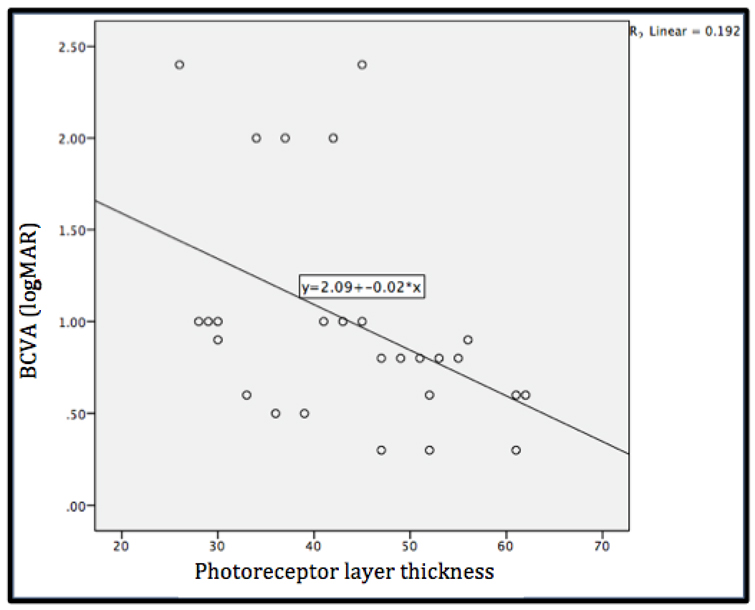
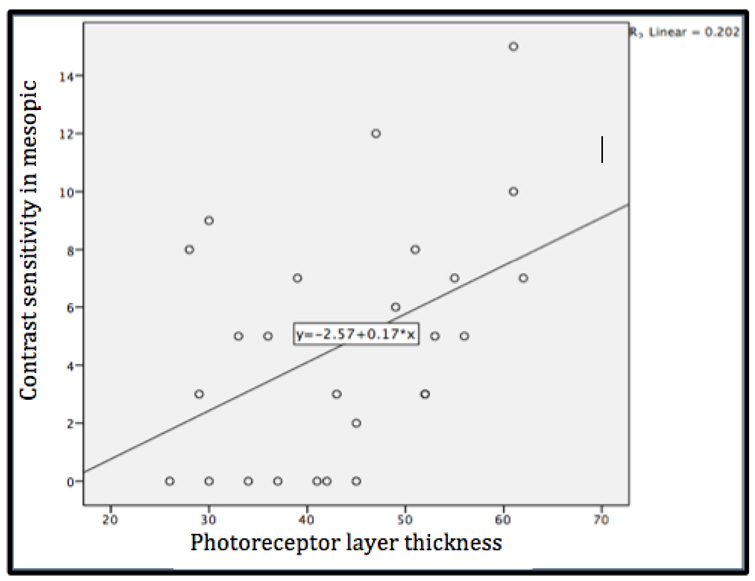
Table 2 reveals there was negative significant correlation between photoreceptor thickness with visual acuity (p value < 0.05) which means the thicker photoreceptor layer gives better visual acuity in logMAR (Figure 2), where best BCVA have lowest logMAR. In Figure 3, similarly with contrast sensitivity in mesopic illumination had positive significant correlation with photoreceptor layer with p value 0.033 (p< 0.05). In contrast, there was insignificant correlation photoreceptor layer with CS in photopic illumination.
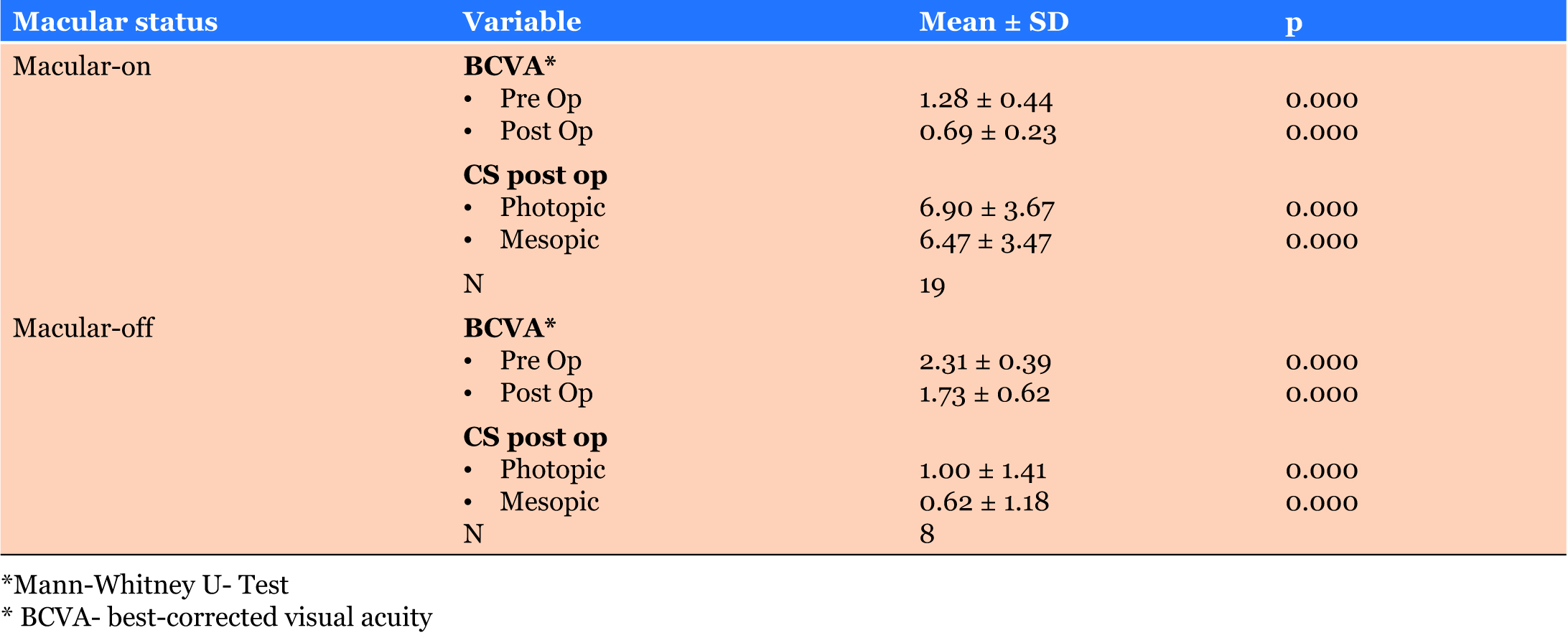
Table 3 consists of comparison visual acuity and contrast sensitivity in mesopic and photopic based on macular status. There was significant difference between BCVA, CS in photopic and mesopic compared between macular-on and macular-off RRD with p value 0.000. Mean visual acuity post-operative in macular-on was 1.73±0.62, while in macular-off was 0.69±0.23. Contrast sensitivity post-operative in photopic illumination had mean 6.90 and 1.00, in macular-on and macular-off RRD, respectively.
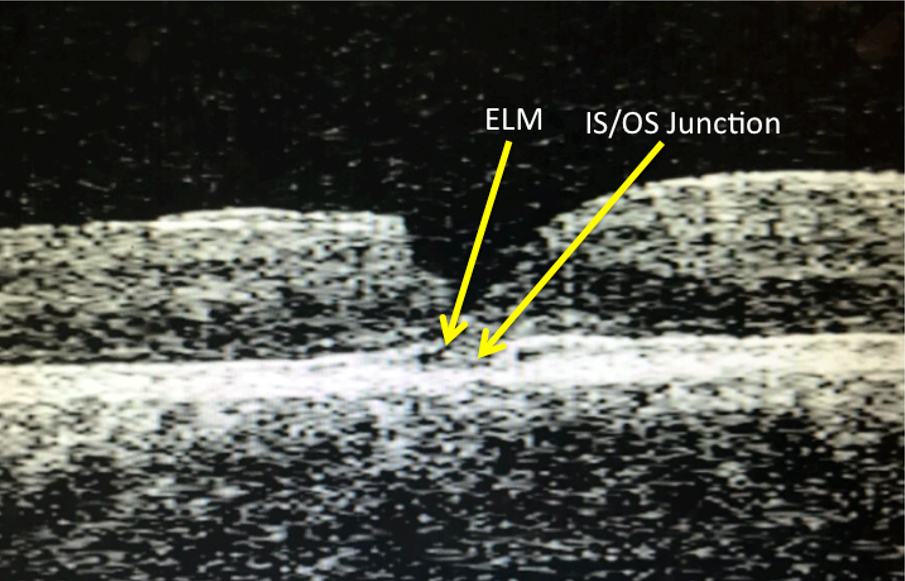
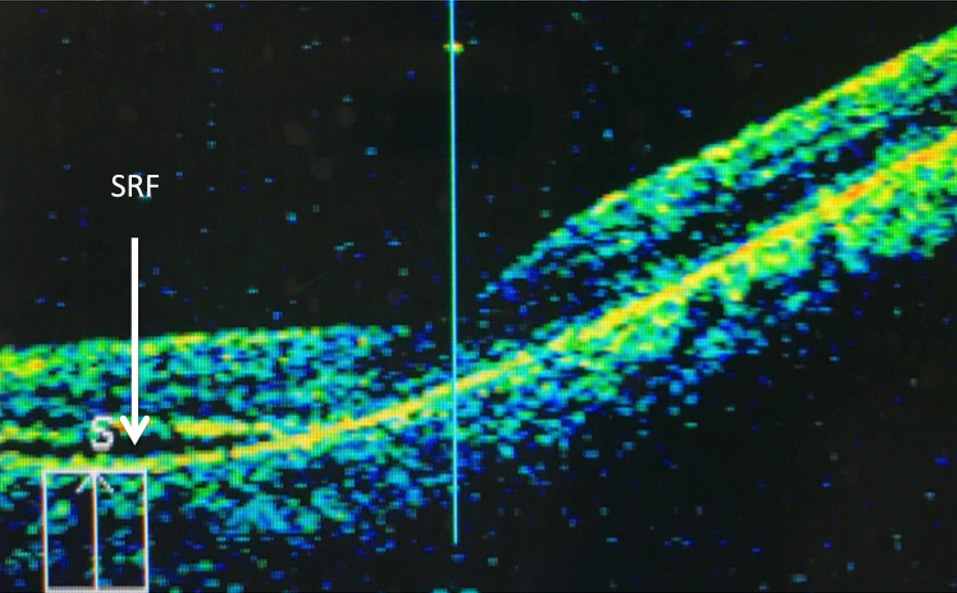
Foveal anatomic abnormalities were detected in six eyes (22.2%), five eyes were in the group macular off RRD, including disruption of the junction between the photoreceptor inner and outer segments (IS/OS) in four eyes, two patients also had a disrupted external limiting membrane (ELM) as shown in Figure 4. One patient with macular on RRD had subretinal fluid who was not detected by indirect ophthalmoscopy, but was detected by the OCT (Figure 5).
DISCUSSION
In our study, there was negative significant correlation between photoreceptor thickness with visual acuity (p value < 0.05) which means the thicker photoreceptor layer gives better visual acuity in logMAR shown in Figure 2, where best BCVA had lowest logMAR. Long term duration of detachment can cause photoreceptor apoptosis, and further it causes neurosensory thinning and dystrophy. The relatively thicker neurosensory of the foveal had a better BCVA compared to the thinner one. Hence, we might conclude that the thinner fovea with macular atrophy had a poor VA, while the thicker one had a better VA. The group with thicker fovea had better VA than the thinner one. Foveal thickness turned thin after retina recovery, it might be due to the cone/rod cell apoptosis. These changes were also detected by OCT.
According to recent studies, a discontinued IS/OS junction was the most frequent lesion, found in 40% to 82% of patients within the photoreceptor layer, and was described as a marker of poor prognosis for visual recovery [17],[18],[19]. Lai and associates reported that the presence of one or more abnormalities among the ELM, the IS/ OS junction, or the Verhoeff membrane was correlated to poor postoperative BCVA [20]. In our study, IS/OS lesions were detected in five subjects eyes. Wakabayashi and his associates noted a disrupted IS/OS junction in 43% of 51 macula-off eyes and found that the integrity of both the ELM and the IS/OS junction was significantly associated with better visual outcome [19]. Final visual acuity in our study, did not differ between patients with simultaneous IS/OS and ELM disruptions and patients with IS/OS disruption and intact ELM. Terauchi et al also demonstrated that photoreceptor abnormalities persisted a long time after surgery. Twenty of 30 eyes (66.7%) had photoreceptor damage that was extended from the outer segments to the outer nuclear layer through the IS/OS [21].
Terauchi findings clearly showed that the IS and OS thicknesses increased in parallel with the improvement of the BCVA after successful retinal reattachment. The results showed that the IS and OS thickness were thin soon after the retina was reattached, and there was an increase in the thickness with increasing time [21].
Visual acuity and contrast sensitivity in photopic and mesopic condition with macular on history of RRD better than macular off with p value 0.00 in this study. Okamoto et al. demonstrated that CS decreased significantly after surgery for macular-on RRD without postoperative complications and abnormal OCT findings. Collectively, these findings indicate that surgical stress could cause a reduction in postoperative CS [22]. However, in our study, the difference in CS was between the macular-on and the macular-off group, possibly suggesting that reduced CS is due rather to foveal detachment than to surgical stress.
Ozgur et al. investigated macular function in eyes with successfully repaired macular-off RRD. They found that CS was lower in the operated eyes than in the fellow eyes. Since their studies included patients with lower postoperative BCVA, they concluded the low CS may have been caused by diminished visual acuity [16]. However, in our study CS was reduced even in eyes with visual acuity of logMAR 0.3 after PPV for RRD. Best corrected visual acuity measurement is the most common test used to evaluate visual function. However, a recent improvement in outcomes of RRD surgery requires a more precise method of visual function testing than BCVA measurement. Although central visual function can be evaluated by several tests including CS measurement, electroretinogram, and central visual field analysis, CS measurement is one of the least invasive, safest, and minimal time consuming. Taken together, the data indicate that CS can be a useful examination for multidimensional evaluation of postoperative visual function [16].
Microscopic changes after successful retinal reattachment with the regeneration process analyzed using animal model and resulted that the length of the outer photoreceptor segments gradually increases depending on the duration of retinal detachment and time since reattachment. The strongest regeneration was observed in eyes with the shortest detachment period and the longest interval between the reattachment and the morphological examination. Cone and rod regeneration processes differ, in cone regeneration, greater variability of outer segment length and generally lower regeneration potential was observed [23].
The topographic variability of changes in reflectivity patterns observed in our study may be associated with the differences between the cone and rod regenerative processes. The processes leading to increased reflectivity of the IS/OS start within the peripheral macula, where rods predominate, and gradually shift towards the center. At the same time, hyper reflective areas begin to appear within the central fovea, where only cones are present. These areas are initially small and tend to progress toward the peripheral macula [23]. Based on the established theory, that should be photopic contrast sensitivity had significant correlation with photoreceptor layer thickness, as cone plays important role in photopic illumination. In contrast, our study revealed that contrast sensitivity in mesopic illumination had positive significant correlation with photoreceptor layer thickness, presumably that pupil more dilated in mesopic condition, and rod predominates in peripheral macula.
This study had some limitations that included different instrument or chart from previously report, therefore it was difficult to compare this study results with other studies. The sample size was small. The method was cross sectional, that could only measure in once follow up. A future larger study with normal control and longer follow up is needed to confirm these findings and to better understand the morphologic and functional changes associated with RRD and subsequent recovery.
CONCLUSION
In conclusion, photoreceptor layer thickness significantly correlated with visual acuity and contrast sensitivity in mesopic illumination. The thicker the photoreceptor, the better visual acuity and mesopic contrast sensitivity was observed.
Henceforth, we strongly recommend OCT for patients whose retina had anatomic reattachment successfully, but achieved VA was not so good. Applying OCT makes it possible to find out the reason of poor VA, even long period of time after operation. This study may provide useful guidelines for the clinical management of retinal detachment as well as for assessing the potential possibilities of visual recovery of patients after successful vitrectomy pars plana.
REFERENCE
1.
Tani P, Robertson DM, Langworthy A. Prognosis for central vision and anatomic reattachment in rhegmatogenous retinal detachment with macula detached. Am J Ophthalmol 1981;92(5):611–20. [CrossRef]
[Pubmed]

2.
Theodossiadis PG, Georgalas IG, Emfietzoglou J, et al. Optical coherence tomography findings in the macula after treatment of rhegmatogenous retinal detachments with spared macula preoperatively. Retina 2003;23(1):69–75.
[Pubmed]
3.
Salicone A, Smiddy WE, Venkatraman A, Feuer W. Visual recovery after scleral buckling procedure for retinal detachment. Ophthalmology 2006;113(10):1734–42. [CrossRef]
[Pubmed]
4.
Ozgür S, Esgin H. Macular function of successfully repaired macula-off retinal detachments. Retina 2007;27(3):358–64. [CrossRef]
[Pubmed]
5.
Cleary PE, Leaver PK. Macular abnormalities in the reattached retina. Br J Ophthalmol 1978;62(9):595–603.
[Pubmed]
6.
Bonnet M, Bievelez B, Noel A, Bensoussan B, Pingault C. Fluorescein angiography after retinal detachment microsurgery. Graefes Arch Clin Exp Ophthalmol 1983;221(1):35–40.
[Pubmed]
7.
Sabates NR, Sabates FN, Sabates R, Lee KY, Ziemianski MC. Macular changes after retinal detachment surgery. Am J Ophthalmol 1989;108(1):22–9.
[Pubmed]
8.
Kishi S, Takahashi H. Three-dimensional observations of developing macular holes. Am J Ophthalmol 2000;130(1):65–75. [CrossRef]
[Pubmed]
9.
Kumagai K, Hangai M, Furukawa M, Larson E, Ogino N. Three-dimensional foveal shape changes after asymptomatic macular posterior vitreous detachment. Clin Ophthalmol 2013;7:751–6. [CrossRef]
[Pubmed]
10.
Pires I, Santos AR, Nunes S, Lobo C. Macular thickness measured by stratus optical coherence tomography in patients with diabetes type 2 and mild nonproliferative retinopathy without clinical evidence of macular edema. Ophthalmologica 2013;229(4):181–6. [CrossRef]
[Pubmed]
11.
Passemard M, Lafontaine PO, Creuzot-Garcher C. Persistent foveal retinal detachment after successful rhegmatogenous retinal detachment surgery by scleral buckling. [Article in French]. J Fr Ophtalmol 2007;30(4):e10.
[Pubmed]
12.
Veckeneer M, Derycke L, Lindstedt EW, et al. Persistent subretinal fluid after surgery for rhegmatogenous retinal detachment: Hypothesis and review. Graefes Arch Clin Exp Ophthalmol 2012;250(6):795–802. [CrossRef]
[Pubmed]
13.
Baba T, Hirose A, Moriyama M, Mochizuki M. Tomographic image and visual recovery of acute macula-off rhegmatogenous retinal detachment. Graefes Arch Clin Exp Ophthalmol 2004;242(7):576–81. [CrossRef]
[Pubmed]
14.
Kawamura H, Fujikawa M, Sawada O, Sawada T, Saishin Y, Ohji M. Contrast sensitivity after pars plana vitrectomy: Comparison between macula-on and macula-off rhegmatogenous retinal detachment. Ophthalmic Res 2016;56(2):74–8. [CrossRef]
[Pubmed]
15.
Leat SJ, Woodhouse JM. Reading performance with low vision aids: Relationship with contrast sensitivity. Ophthalmic Physiol Opt 1993;13(1):9–16.
[Pubmed]
16.
Ozgür S, Esgin H. Macular function of successfully repaired macula-off retinal detachments. Retina 2007;27(3):358–64. [CrossRef]
[Pubmed]
17.
Smith AJ, Telander DG, Zawadzki RJ, et al. Highresolution fourier-domain optical coherence tomography and microperimetric findings after macula-off retinal detachment repair. Ophthalmology 2008;115(11):1923–29. [CrossRef]
[Pubmed]
18.
Nakanishi H, Hangai M, Unoki N, et al. Spectraldomain optical coherence tomography imaging of the detached macula in rhegmatogenous retinal detachment. Retina 2009;29(2):232–42. [CrossRef]
[Pubmed]
19.
Wakabayashi T, Oshima Y, Fujimoto H, et al. Foveal microstructure and visual acuity after retinal detachment repair: Imaging analysis by fourier-domain optical coherence tomography. Ophthalmology 2009;116(3):519–28. [CrossRef]
[Pubmed]
20.
Lai WW, Leung GY, Chan CW, Yeung IY, Wong D. Simultaneous spectral domain OCT and fundus autofluorescence imaging of the macula and microperimetric correspondence after successful repair of rhegmatogenous retinal detachment. Br J Ophthalmol 2010;94(3):311–18. [CrossRef]
[Pubmed]
21.
Terauchi G, Shinoda K, Matsumoto CS, Watanabe E, Matsumoto H, Mizota A. Recovery of photoreceptor inner and outer segment layer thickness after reattachment of rhegmatogenous retinal detachment. Br J Ophthalmol 2015;99(10):1323–7. [CrossRef]
[Pubmed]
22.
Okamoto F, Okamoto Y, Hiraoka T, Oshika T. Vision-related quality of life and visual function after retinal detachment surgery. Am J Ophthalmol 2008;146(1):85–90.
23.
Anderson DH, Guérin CJ, Erickson PA, Stern WH, Fisher SK. Morphological recovery in the reattached retina. Invest Ophthalmol Vis Sci 1986;27(2):168–83.
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Andi Muhammad Ichsan - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Andi Suryanita Tajuddin - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Habibah Setyawati Muhiddin - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Budu - Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Batari Todja Umar - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Noro Waspodo - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Andi Muhammad Ichsan et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



