 |
Case Report
Herpetic endotheliitis following an uncomplicated cataract surgery
1 Regional Military University Hospital of Constantine, BP 61, Ali Mendjeli, Constantine, Algeria, University of Constantine 3, Algeria
Address correspondence to:
Saad Leboukhe
MD, PhD, Regional Military University Hospital of Constantine, BP 61, Ali Mendjeli, Constantine, Algeria, University of Constantine 3,
Algeria
Message to Corresponding Author
Article ID: 100005O02SL2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Leboukhe S, Relila M. Herpetic endotheliitis following an uncomplicated cataract surgery. Edorium J Ophthalmol 2021;4:100005O02SL2021.ABSTRACT
Introduction: Herpetic endotheliitis after cataract surgery is a rare complication, and it is more likely linked with previous ocular herpetic infection.
Case Report: In the current case, the patient of this study is a 66-year-old woman without a personal history of herpes simplex keratitis (HSK) who underwent an uneventful phacoemulsification in her left eye. For the next two weeks, corneal endotheliitis appeared in the same eye, and then the initial diagnosis of HSK was made clinically. The patient was treated with systemic and topical antiviral therapy associated with an intensive topical corticosteroid. In four weeks, a complete resolution of the corneal edema was noticed and the visual acuity was improved (6/9).
Conclusion: The occurrence of corneal edema after cataract surgery could reveal a herpetic endotheliitis, although early diagnosis and early treatment with strict monitoring are the keys to successful control of this affection.
Keywords: Cataract surgery, Corneal endotheliitis, Simplex herpetic virus
INTRODUCTION
Corneal endotheliitis is a serious condition in which the inflammation affects the endothelium at first [1]. It is and could be the subject of many viral infections, such as herpes simplex virus type 1 (HSV1), cytomegalovirus (CMV), varicella zoster virus (VZV), and Epstein–Barr virus (EBV) [2]. The mechanism of this disease could be connected directly to the virus infection or to the immune system response [3].
As a consequence, this biologic phenomenon leads to a corneal edema, a keratic precipitates (KP), and a minimal anterior chamber inflammation as well [1].
Increase in intraocular pressure (IOP), inflammatory changes within the corneal stroma and corneal hypoesthesia are the characterized signs of this affection [2]. Endotheliitis is classified into linear, sectoral, disciform, and diffuse subgroups [2].
Ocular surgery, eye trauma, febrile illness, and psychological stress play the main role that lead to the herpes simplex virus type 1 (HSV1) reactivation [4].
Recent studies have reported a number of cases which herpetic endotheliitis is caused by a cataract surgery, but these cases remain exceptional [5].
In this article, we will report and discuss the case of herpetic endotheliitis following uncomplicated cataract surgery.
CASE REPORT
We report the case of a 66-year-old woman without any personal health history, whether medical or surgical, referred to our department at the Military University Hospital of Constantine for a progressive vision loss in her left eye (6/60). Slit lamp examination of the same eye had shown a clear cornea without any epithelial, stromal, or endothelial abnormalities. A corticonuclear cataract grade II was noticed. The rest of the clinical exam, including the eye fundus, did not let out any abnormalities.
The patient was operated in our department by uneventful phacoemulsification surgery including lens implantation. The cornea was clear and lucid on the first day following the surgery. After seven days the final uncorrected visual acuity was 6/9.
After a week, the patient came to our emergency room for a cloudy vision in her left eye associated with redness and photophobia. These symptoms started 48 hours back. The vision was decreased to hand movement at 50 cm. The corneal examination making use of a slit-lamp after a corneal fluorescein eye stain test did not show any epithelium abnormalities.
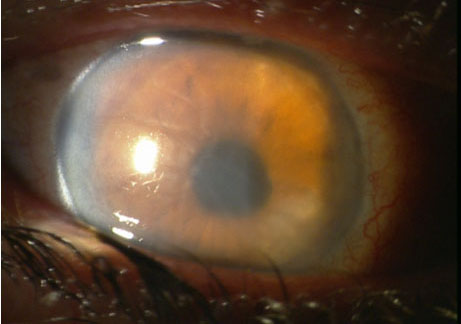
Diffuse stromal edema, Descemet membrane folds, retro-corneal pigmentation with eight dense deposits, and a mild anterior chamber inflammation were perceived and noticed. The number of visible cells limited to 10 cells/field.
The number of cells was calculated according to the standard of uveitis nomenclature working group grading scheme for anterior chamber cells.
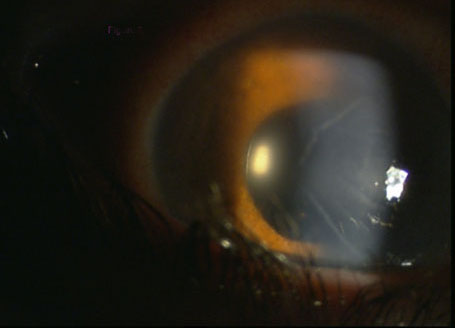
Figure 1 and Figure 2 demonstrate some of these clinical signs. Intraocular pressure (IOP) measured and adjusted according to the corneal pachymetry was (12 mmHg) in the right eye and (30 mmHg) in the left. Also, corneal hypoesthesia was more remarkable in the left eye compared to the right eye.
Corneal thickness was respectively measured in the right (545 μm) and the left eye (689 μm), utilizing an optical coherence tomography (OCT, Heidelberg, Germany).
According to these findings, a presumed diagnosis of herpetic endotheliitis was made and the patient was treated by systemic and topical antiviral therapy associated with topical corticosteroid according to the protocol mentioned in the Medico-Surgical Encyclopedia 2014 [6].
- Intravenous Acyclovir: 8 mg/kg every 8 hours per day for one week.
Local treatment:
- 0.15% Ganciclovir eye gel: four times per day.
- 0.1% Dexamethasone eye drops: hourly (every hour) after amelioration and improvement.
- 0.5% Timolol eye drops: once a day at 8 A.M.
- 1% Atropine sulfate eye drops: three times a day.
In a week, corneal edema was recovered and recuperated remarkably (Figure 2), visual acuity was improved considerably (6/18) as well. At that point, we have stopped the systemic antiviral Acyclovir for the patient, and replaced it by the oral Acyclovir 400 mg five times a day, besides were reduced Dexamethasone eye drops progressively.
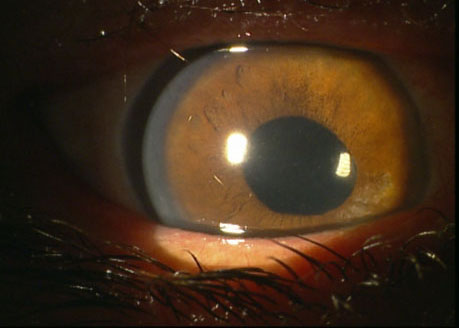
In four weeks, a complete resolution of the corneal edema was greatly noticed (Figure 3) and also the visual acuity was improved considerably (6/9). 800 mg per day of Acyclovir was sustained for one year to prevent reappearances and recurrences once again.
DISCUSSION
The endothelium could be, most likely the first site of secondary inflammation caused by herpes simplex virus type 1 (HSV1) reappearance or recurrence after cataract surgery, the cause of herpetic endotheliitis. Even patients with a healthy personal history which exclude any symptoms of herpetic infection could be affected [7].
The complication of herpes recurrence is related to the harshness and virulence of the immune system response due to the virus [4]. The viral reactivation is correlated to the injury, referring to the sub-epithelial plexus of trigeminal nerves during cataract incision and the intensive use of topical corticosteroids after the surgery [8].
The reactivation of HSV1 within the endothelium after uncomplicated cataract surgery is a phenomenon that has been described by many authors [9],[10]. We take as an example: Haiou Wang, in a multicentric study involving 22,935 patients, who underwent cataract surgery with no previous herpetic infection, reported an incidence of 0.28% of herpetic endotheliitis and noted two main risk factors, which are: old age and diabetes [11]. The onset time of reactivation of the virus in the current case (one week) is within the range of published data from 5 days to 5 weeks after surgery [7],[9],[11],[12].
Many viruses are implicated in the viral endotheliitis; 95% are related to ocular HSV1 [3],[13]. Also, it is essential to mention that viral culture and polymerase chain reaction (PCR) are not sensitive enough to prove the viral etiologies because 55% of tests could be negative [14],[15]. In this case, PCR was not conducted (due to lack of facilities for the test in the hospital laboratory). Accordingly, the diagnosis of herpetic endotheliitis was made clinically. The complete resolution of signs and symptoms using Acyclovir as a treatment confirms over and over the origin of the herpetic viral infection [11],[16].
Although cytomegalovirus (CMV) endotheliitis after cataract surgery shares the same clinical signs as herpetic endotheliitis, many parameters may help to distinguish between them. In the case of the cytomegalovirus (CMV) infection, it is more prevalent in the Asia Pacific rather than in other countries [17], the diffuse corneal edema (CMV) is rare compared to herpetic infection [16] also the topical and systemic therapeutic test to Acyclovir treatment is less efficient comparing to herpetic endotheliitis which responses rapidly and favorably. In this case of cytomegalovirus (CMV) endotheliitis, the Valacyclovir is the best choice for the treatment [18].
The surgical conditions like hard cataract, weak dilatation, and ultrasound phacoemulsification overuse represent one of the corneal edema causes after cataract surgery [19],[20],[21]. In this case, corneal edema should be seen already on the first day during the monitoring. On the contrary, the onset of secondary edema caused by a viral infection is between five days and five weeks [7],[9],[11]. According to this fact, we believe that the first day of monitoring following cataract surgery is priceless because the detection of corneal edema on the first day could help find out the viral infection.
Unfortunately, some cases which are misdiagnosis or not treated rapidly could lead to corneal endothelial decompensation. In such a case, Descemet Membrane Endothelial Keratpolasty or DMEK surgery is the best choice to rehabilitate those patients, but it is followed by a high risk of herpetic recurrence [22]. The utilization of intensive antiviral therapy before, during, and long after surgery is necessary [23].
CONCLUSION
Corneal edema sequential to a cataract surgery could reveal the herpetic endotheliitis, the fact remain that its clinical features are easily recognized but it could be confused with further pathologies. Ophthalmologists should be aware and more attentive even for patients without herpetic infection history, where in that case, PCR might be helpful. Early diagnosis and early treatment with a strict and a serious monitoring are the keys to a successful control of this affection.
REFERENCE
1.
Khodadoust AA, Attarzadeh A. Presumed autoimmune corneal endotheliopathy. Am J Ophthalmol 1982;93(6):718–22. [CrossRef]
[Pubmed]

2.
Suzuki T, Ohashi Y. Corneal endotheliitis. Semin Ophthalmol 2008;23(4):235–40. [CrossRef]
[Pubmed]
3.
Asi F, Milioti G, Seitz B. Descemet membrane endothelial keratoplasty for corneal decompensation caused by herpes simplex virus endotheliitis. J Cataract Refract Surg 2018;44(1):106–8. [CrossRef]
[Pubmed]
4.
Babu MS, Balammal G, Sangeetha G, Krishna LM. A review on viral keratitis caused by herpes simplex virus. J Sci 2011;1:1–10.
5.
Zamir E, Stawell R, Jhanji V, Vajpayee RB. Corneal endotheliitis triggered by cataract surgery in a Chinese patient with cytomegalovirus anterior uveitis. Clin Exp Ophthalmol 2011;39(9):913–5. [CrossRef]
[Pubmed]
6.
Labetoulle M, Rousseau A, Bourcier T. Atteintes herpétiques du segment antérieur de l’oeil: aspects épidémiologiques, cliniques et diagnostiques. EMC Ophtalmologie 2014;[21-200-D-20].
7.
Barequet IS, Wasserzug Y. Herpes simplex keratitis after cataract surgery. Cornea 2007;26(5):615–7. [CrossRef]
[Pubmed]
8.
Cho YK, Kwon JW, Konda S, Ambati BK. Epithelial Keratitis after cataract surgery. Cornea 2018;37(6):755–9.
[Pubmed]
9.
Jhanji V, Ferdinands M, Sheorey H, Sharma N, Jardine D, Vajpayee RB. Unusual clinical presentations of new-onset herpetic eye disease after ocular surgery. Acta Ophthalmol 2012;90(6):514–8. [CrossRef]
[Pubmed]
10.
Vajpayee RB, Sharma N, Verma K, Saxena T, Tandon R. Presumed herpetic endotheliitis following phacoemulsification surgery. Clin Exp Ophthalmol 2006;34(6):617–21. [CrossRef]
[Pubmed]
11.
Wang H, Zheng J, Zheng Q, et al. Incidence and risk factors of new onset endotheliitis after cataract surgery. Invest Ophthalmol Vis Sci 2018;59(12):5210–6. [CrossRef]
[Pubmed]
12.
Patel NN, Teng CC, Sperber LTD, Dodick JM. New-onset herpes simplex virus keratitis after cataract surgery. Cornea 2009;28(1):108–10. [CrossRef]
[Pubmed]
13.
Knickelbein JE, Hendricks RL, Charukamnoetkanok P. Management of herpes simplex virus stromal keratitis: An evidence-based review. Surv Ophthalmol 2009;54(2):226–34. [CrossRef]
[Pubmed]
14.
Kakimaru-Hasegawa A, Kuo CH, Komatsu N, Komatsu K, Miyazaki D, Inoue Y. Clinical application of real-time polymerase chain reaction for diagnosis of herpetic diseases of the anterior segment of the eye. Jpn J Ophthalmol 2008;52(1):24–31 [CrossRef]
[Pubmed]
15.
Shoji J, Sakimoto T, Inada N, et al. A diagnostic method for herpes simplex keratitis by simultaneous measurement of viral DNA and virus-specific secretory IgA in tears: An evaluation. Jpn J Ophthalmol 2016;60(4):294–301. [CrossRef]
[Pubmed]
16.
Alfawaz A. Cytomegalovirus-related corneal endotheliitis: A review article. Saudi J Ophthalmol 2013;27(1):47–9. [CrossRef]
[Pubmed]
17.
Wong A, Tan KH, Tee CS, Yeo GS. Seroprevalence of cytomegalovirus, toxoplasma and parvovirus in pregnancy. Singapore Med J 2000;41(4):151–5.
[Pubmed]
18.
Anshu A, Chee SP, Mehta JS, Tan DTH. Cytomegalovirus endotheliitis in Descemet’s stripping endothelial keratoplasty. Ophthalmology 2009;116(4):624–30. [CrossRef]
[Pubmed]
19.
Sharma N, Singhal D, Nair SP, Sahay P, Sreeshankar SS, Maharana PK. Corneal edema after phacoemulsification. Indian J Ophthalmol 2017;65(12):1381–9. [CrossRef]
[Pubmed]
20.
Kausar A, Farooq S, Akhter W, Akhtar N. Transient corneal edema after phacoemulsification. J Coll Physicians Surg Pak 2015;25(7):505–9.
[Pubmed]
21.
Costagliola C, Romano V, Forbice E, Angi M, Pascotto A, Boccia T, et al. Corneal oedema and its medical treatment. Clin Exp Optom 2013;96(6):529–35. [CrossRef]
[Pubmed]
22.
Abdelmassih Y, Dubrulle P, Sitbon C, et al. Therapeutic challenges and prognosis of descemet’s membrane endothelial keratoplasty in herpes simplex eye disease. Cornea 2019;38(5):553–8. [CrossRef]
[Pubmed]
23.
Friehmann A, Myerscough J, Giannaccare G, Mazzoni M, Bovone C, Busin M. Successful descemet membrane endothelial keratoplasty in proven herpetic endothelial decompensation requires intensive antiviral therapy. Cornea 2020;39(2):196–9. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Saad Leboukhe - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Mounir Relila - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Saad Leboukhe et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


